|
Case histories > PABRLN
Paralysis of the anterior branch of the recurrent laryngeal nerve (PABRLN)
History
- 6th decade
- female
- Pneumonia
- Began losing voice two weeks later
- diagnosed with left complete vocal paralysis
- MRI 2 months after injury: no lesions of recurrent nerve, atrophy of left intrinsic laryngeal muscles
- 4 months after initial injury gelfoam injection improved voice
- 5 months after initial injury movement is returning
- 1 year post injury she notes the following
- hoarseness
- throat discomfort and tightness after talking
- cannot yell
- poor vocal endurance
- breakup of voice when singing in the middle of her range
- Occupation: music teacher
Character
- talkativeness scale: 5
- loudness: 4
Vocal capabilities
- Reading voice
- intermittent breakups
- diplophonia
- Pitch range
- Anchor pitch (F0) - F3
- Low pitch - C3
- High pitch - C6+
- swelling test (onset delays and breathiness) - none, voice actually clearer at higher pitches
- Singing - G4 - flutter with soft singing
- Maximum phonation: at F3 is >12 seconds
- Loudness: excellent
Laryngoscopic Examination
|

|
- Adduction - left vocal fold goes through a shorter range of motion and remains slightly abducted
- Vocal processes oppose, though not symmetrically
- Strobe - asymmetry of mucosal wave, perhaps 90 degrees out of phase, intermittent diplophonia degrades strobeoscopic exam
- Left subglottic conus atrophic
- Left vocal process angled outward
- Left vocal fold slightly bowed at rest
- Click to see a more detailed set of photos
|
|
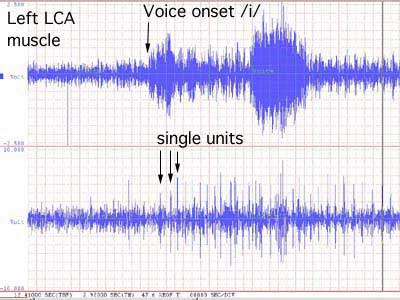
EMG Click to see full set of EMG recordings.
|